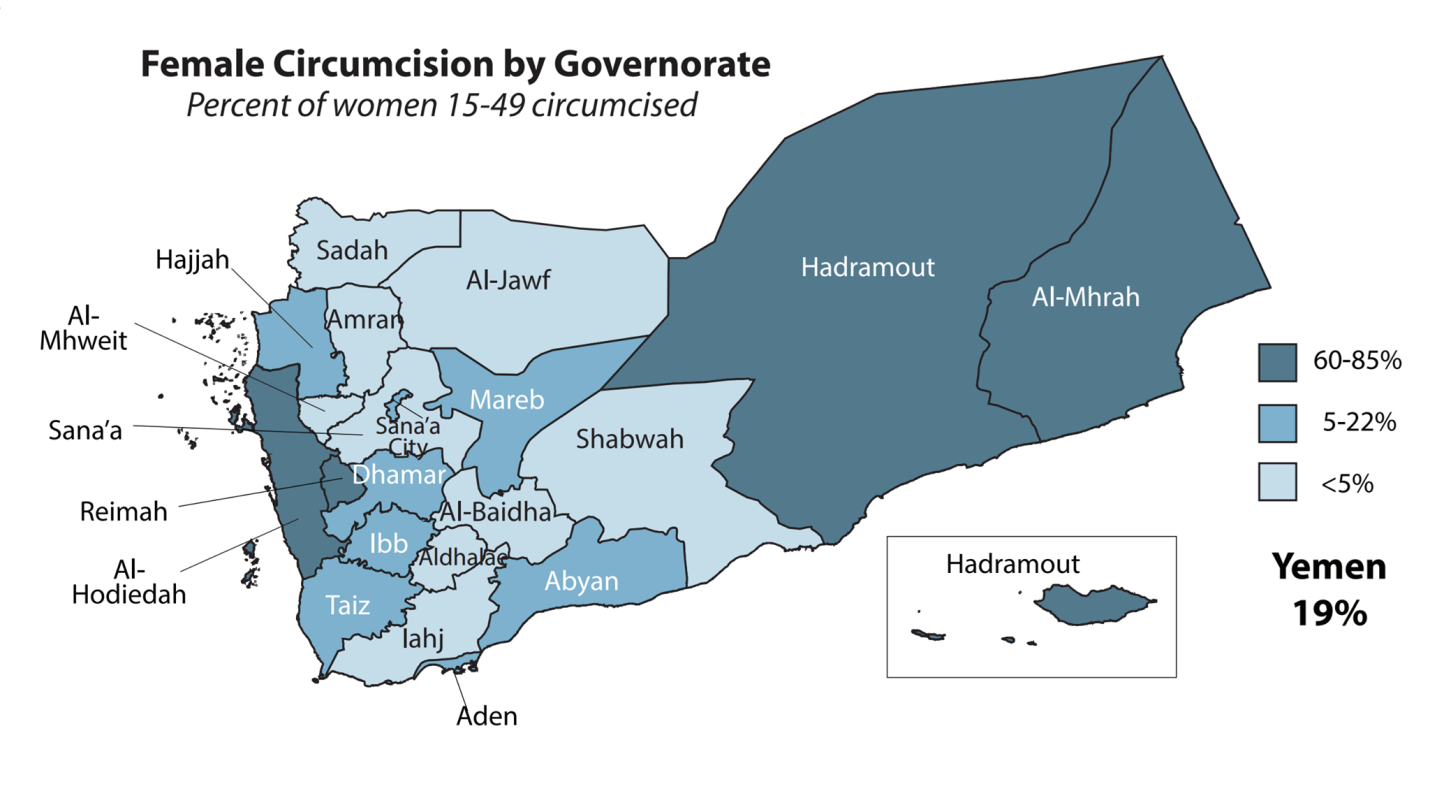
FGM in Yemen is distributed throughout the country but predominates in four main cities; Aden, Al-Hodiedah, Al-Mhrah, and Hadramout. In 2001, the Yemeni Ministry of Public Health and Population (YMoPHP) enacted a decree to ban public and private health facilities from performing FGM. However, some facilities still carry out the practice. Therefore, a study of the determinates that make families and communities mutilate their girls is mandatory. Appropriate, concurrent interventions to address these determinants are critical for FGM to be eliminated in Yemen.
FGM Determinants Analysis in Yemen:
1-Intrapersonal Determinants:
FGM in Yemen is carried out as a result of commonly held cultural and religious beliefs, often inherited from the family or community members. 86% of mothers and grandmothers believe that it is a cleaning and purity practice for the female genitalia. This was elaborated in a study by the YMoPHP with 35% of women saying FGM practice should continue. Most of these women were illiterate or from rural areas: women’s education in Yemen is poor in general with 42% of women being illiterate, whereas only 19% have correct information of the harm of FGM. Interestingly, 65% of men are against FGM. The Yemeni medical education and training curriculum has no information about FGM. Therefore, public and private practitioners are not educated about FGM and its harmful consequences for women’s health.
2-Interpersonal Determinants:
Elimination of FGM is resisted by women themselves as members who support the practice in these areas are often mothers and grandmothers. Many girls who underwent FGM had the surgery done at their homes by a traditional FGM practitioner or their grandmothers. Several studies showed that most of the time FGM occurs without the fathers’ Knowledge. Women’s friends and peers often support the practice, whereas men’s friends and peers oppose it. Survey interviews pointed out that 58% of men reported that they do not want to marry a mutilated woman as they would not be able to enjoy the sexual intercourse. This enforces the need to engage Yemeni men in interventions and advocacy campaigns in Yemen.
3-Community Determinants:
The geographical location of these four communities brings about another determinant: the warm climate is considered to increase sexual desire, resulting in the belief that FGM would protect their girls from premarital sex and suppress their sexual needs. Many mothers believe that FGM will make girls marriageable and encourage their sons to marry only FGM girls as it indicates their virginity. Curiously, many women still do not consider that FGM is the reason that girls are not enjoying intercourse with their husbands.
Other geographical areas shown to have FMG cases contain families who migrated there or which have relatives from the four main areas in this study.
4-Institutional Determinants:
The enforcement of policy or sanctions for practitioners (professional and traditional) who carry out FGM have never been applied. Ostensibly, traditional medical practitioners including Traditional Birth Attendants (TBAs) still have a high influence and people count on them in rural areas. Traditional FGM practitioners are most common and often gained their skills from grandmothers. However, they often use unclean tools that can risk the baby girl’s life and they do not have the necessary experience to manage complications.
On the other hand, the absence of registration of girls’ deaths related to FGM should be enforced in health facilities. This would facilitate the gathering of evidence for policymakers, reinforce the importance of the issue and support robust public policy or measures to eliminate FGM.
5-Public Policy Determinants:
A law to ban the practice is still on hold in the Yemeni parliament as the Shari’a committee (a group of religious leaders who announce religious statements for the public and the country) still believe that it is a religious practice or custom of these communities. However, committee members are unfamiliar with the harmful consequences of FGM on women’s health because they have not been adequately involved in interventions or campaigns. In addition, advocates have not been provided with sufficient evidence to present to the committee and other policymakers.
Interventions and Policies to Eradicate FGM in Yemen:
To address the issue appropriately and effectively, broad interventions and policies need to be implemented. Interventions and policies should include three components to achieve a holistic approach: health education, service delivery, and structural factors. Moreover, as an issue that has religious and cultural impulses, the integration of key members of the community is essential to change behaviour and/or belief.
1-Health Education:
- Traditional FGM Practitioners:
Traditional FGM practitioners should be targeted and empowered to give up the practice. In Egypt and Kenya, practitioners were targeted in awareness campaigns to highlight the harm of the practice and enable them to educate the communities who approach them. They even assisted them with training to become TBAs in order to enhance their skills as part of the supportive environment to ultimately eliminate the practice. In Yemen, this would immensely enable the elimination process and empower those practitioners to cease FGM.
- Imams (Religious Leaders):
Religious leaders’ endorsement is significant in this issue. Imams can raise the awareness about the harm of FGM during their religious sermons to enable the male community to stop the practice. In Kurdistan, Iraq, community initiatives engaged religious leaders to educate them about the harm of the practice. Subsequently, a Fatawa (Religious Statement) was declared in 2010 in Kurdistan that FGM is not part of Islam. In Yemen, this could tremendously influence FGM abolishment as many communities trust their religious leaders and follow their statements.
- Media Campaigns:
The media can shape debates about controversial health issues and lead the public to start thinking about them. It could facilitate a change in attitude towards FGM practice and its short and long term effects. In such a conservative country as Yemen, and with such a taboo issue, radio would be the most appropriate and effective tool. Radio would be the most accessible medium for people who are not visiting health facilities or who are literate. It would also reach those hidden traditional FGM practitioners to educate and inform them about FGM elimination campaigns and how they can join them. In Burkina Faso, radio campaigns on the harm of FGM reduced the practice by 28%.
- Information Dissemination:
There is a need to incorporate FGM information within the education system. It would raise awareness about the practice and correct the misconception of its advantages to girls’ and womens’ reproductive and personal hygiene. Schools, universities, and even street campaigns would increase awareness and emphasize the harm of FGM to girls’ and women’s reproductive and sexual health. Sessions and posters should be supplied in health facilities as part of the FGM information dissemination campaigns.
2-Service Delivery:
- Public and Private Practitioners:
Actions for women’s health should be carried out by TBAs and hospital health professionals in each district. Training should be established for practitioners in public and private facilities, especially in the aforementioned four cities in Yemen where FGM is high. Training should also remind them of their role in the medical field and the oath they made to save peoples’ lives.
- Traditional FGM Practitioners:
Training should enable them to develop new skills and encourage them to turn away from FGM. FGM practitioners can become advocates against FGM in their communities. Evidently, communities trust traditional FGM practitioners and would follow their guidance and advice. Intervention like this have proven success in countries such as Egypt and Kenya. In Yemen, it would play an integral role as FGM is mostly done by those practitioners.
- Training at Homes for Grandmothers and Mothers:
Re-trained traditional FGM practitioners (those who become TBAs) should carry this massage to their communities. This would significantly enable the grandmothers and mothers to absorb the information as they have their trust. Therefore, re-trained traditional FGM practitioners and grandmothers are essential for FGM eradication in Yemen.
- Counselling and Support:
The need to empower FGM victims is another area that has not been considered. Training and counselling for victims need to be implemented as part of the wider motivation for a behavioural change in the upcoming generation in Yemen. Psychosocial specialists in schools also could identify and help those in need, which will in turn increase health literacy in future generations. In Egypt, most of the volunteers working to prevent FGM are FGM victims who were trained and empowered. Similarly, victim empowerment in Yemen would make a huge difference to abolish FGM.
3-Structural Factors:
- Advocacy:
1- Registration of FGM deaths would provide evidence of the significance of the issue for community, religious, and state leaders.
2- Enforcement of the 2001 decree with sanctions on healthcare practitioners (professional and traditional) who disobey.
3- Amendment of the decree to include supervision rounds to evaluate health facilities for their promotion of the harm of FGM.
4- Victim stories and community figures’ interviews should be included in the radio campaigns. This would highlight the negative effects of FGM on women’s health and equally help to raise the self-efficacy among them.
- Policy:
1- A rigorous law would emerge if the evidence by the advocacy campaigns above could successfully be provided. Religious, community, and state leaders’ involvement in advocacy campaigns is critical to maintain their support and endorsement.
2- Multisectoral partnerships should be developed to address health issues. Therefore, putting FGM in the country agenda would establish multisectoral measures to abolish the practice.
3- As Yemen is part of the child rights and the elimination of Women’s Discrimination Convention. It imperatively stress the policymakers’ attention towards FGM as it is a critical child/women’s right issue.
FGM is not just a health issue that can be repaired, it is a life taken from those girls and women that we cannot bring back unless we put an end to this barbaric and unnecessary practice.

[…] 9- Female Genital Mutilation (FGM) in Yemen – A study of FGM determinants and approaches to add… […]